
GIRD - Friend or Foe
GIRD is a common term that is thrown around in baseball, and it can sometimes carry quite the negative connotation. I have had plenty of ball players come into my office and say, “I have GIRD,” or “I was diagnosed with GIRD” like they’ve just sustained a devastating injury. On the other hand I have had players ask how to get GIRD, thinking that if they get it they will perform better.
I believe both of these viewpoints come from a place of misunderstanding GIRD and how it affects the shoulder. In this post we will address what is GIRD and why does it happen? We will also examine if it is an actual issue or not, and if it is, what to do about it. Let's get started.
What is GIRD?
GIRD stands for Glenohumeral Internal Rotation Deficit. The acronym describes the process in which a thrower loses their internal rotation (IR), and then usually gains external rotation (ER). Your average person will have 90 degrees of both internal and external rotation (totaling in 180 total degrees), but it is not unusual for a baseball player to have 65 degrees of internal rotation and 115 degrees of external rotation (still totaling 180 degrees). This change in motion is called GIRD.
Now, this phenomenon is actually a normal process that happens with all baseball pitchers to some degree. In addition, this adaption is advantageous. Think of it like a slingshot. The further you can pull the ball back, the faster you can propel it forward. The shoulder is build for 180 degrees of rotation, so in order to pull the slingshot back further the shoulder adapts. A trade is made. The athlete gains ER, and loses IR.
So now that we know GIRD is normal and advantageous, why exactly does it happen?
There are 3 leading explanations for why GIRD occurs.
Humeral Retroversion
Posterior Capsule Stiffness
Posterior Soft Tissue Tightness
Humeral Retroversion starts when we grow up playing little league. As we expose our shoulder to the demands of throwing the body adapts to help us out. Since gaining ER is good for throwing, our bones actually morph as we grow to allow for more ER. The research shows that our bones can adapt and allow for an extra 12-15 degrees of ER. Elite pitchers in the MLB have seen up to 20 degrees. This is a testament to just how adaptable our body can be. However adding 12-15 degrees does not fully explain for pitchers having 120 degrees of ER, other factors have to be at play.
Throwing a baseball 90+ MPH over the course of innings takes a lot of force. This force results in micro-tearing of the shoulder musculature and joints. As the body heals from this damage some research shows that the backside of the shoulder joint thickens. This increase in thickness reduces the shoulder’s ability to internally rotate. Conversely, there is also research that states that the backside of the shoulder gets too stretched. In research it is not uncommon to have conflicting results, so which one is right here? In my experience ball players usually have loose shoulders, and the posterior capsule stiffness is not typically present. My colleagues who treat baseball players also agree with this.
The micro-tearing also affects the muscles. Pitchers will often point to soreness in the back of the shoulder and at times say it is hard to reach across their body after an outing. Tightness along the back of the shoulder is definitely a common thing I see, and it is well documented in the research. That muscle tightness will then limit IR, and will feel better in the shortened position that is ER.
When is GIRD an Issue?
I already went over how GIRD is normal for a thrower, but then why is it commonly diagnosed alongside injury? There are some instances when GIRD can be problematic. This is when the following criteria is met:
Pain in the shoulder
Loss of 20-25 degrees of IR that is not made up for in ER Gain.
Total Arc of Motion being over 10 degrees less than the other side.
When I have a player walk in meeting this criteria, it is time to treat GIRD. And really, waiting for the pain to onset is a risky move. We want to be as proactive as possible if the 2nd and 3rd criteria are met.
GIRD Case Examples
Let's take a look at 3 baseball players.
Player A pictured here has 110 degrees of External Rotation, and 70 degrees of Internal Rotation. Added together that totals 180 degrees. He also has 180 degrees on his opposite side. In this scenario Player A’s shoulder GIRD is normal, and should not be adjusted.
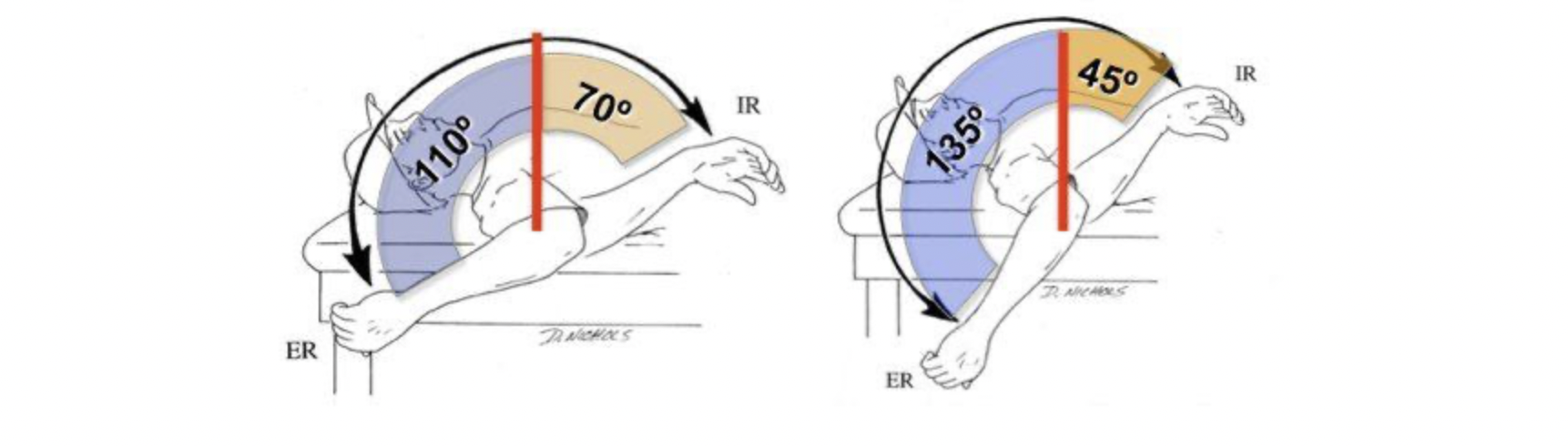
A B
Player B pictured has 135 degrees of External Rotation, and 45 degrees of Internal Rotation. Again, this equals 180 degrees of total motion. He also has 180 degrees on his opposite side. Just like Player A, this pitcher is just fine. The numbers are different, but as long as the total is symmetrical we are not concerned.

C
Player C pictured has 115 degrees of External Rotation, and 40 degrees of Internal Rotation. This sums up to 155 degrees. His opposite shoulder has 180 degrees of motion for rotation. In this scenario Player C is missing 25 degrees of motion when compared to his other side. Player C is now a candidate for treatment.
If Player C’s opposite side motion was also 155 degrees, he would be considered normal.
Treating GIRD
Many clinicians, coaches, and trainers will treat GIRD the same way. They will have the athlete perform a Cross Body Stretch, or another posterior shoulder stretch to try and improve IR.
This is not the way to go about it.
There are several considerations to take into account when deciding what motion to improve. In some cases improving IR is the go to, and stretching plus soft tissue massage is a great option. In others, gaining ER is needed and this can be done by lengthening the muscles that perform IR. The only way to know which direction to take is to be properly assessed.
Get Ahead and Get Assessed
The best way to deal with GIRD is to be knowledgeable about it, and be aware of where you are personally. This can be done by getting an assessment. A trained professional can accurately measure the shoulder to let you know where you sit and if you are in a good spot. This knowledge will help you stay healthy and on the mound performing at your best. This assessment can be done here at Austin Athletic, by our friends at Reach Training, or from another trained individual if you are not in the area.
Sources
Rose, M. B., & Noonan, T. (2018). Glenohumeral internal rotation deficit in throwing athletes: Current perspectives. Open Access Journal of Sports Medicine, Volume 9, 69–78. https://doi.org/10.2147/oajsm.s138975